Applications for the LAMP Fellowship 2025-26 will open on December 1, 2024. Sign up here to be notified when applications open.
On June 1, 2020, the Cabinet Committee on Economic Affairs approved a revision in the definition of Micro, Small and Medium Enterprises (MSMEs).[1] In this blog, we discuss the change in the definition as approved by the Cabinet, and examine some of the common criteria used for classification of MSMEs.
Currently, MSMEs are defined under the Micro, Small and Medium Enterprises Development Act, 2006.[2] The Act classifies them as micro, small and medium enterprises based on: (i) investment in plant and machinery for enterprises engaged in manufacturing or production of goods, and (ii) investment in equipment for enterprises providing services. As per the Cabinet approval, the investment limits will be revised upwards and annual turnover of the enterprise will be used as additional criteria for the classification of MSMEs (Table 1).
Earlier attempts to amend the definition of MSMEs
The central government has sought to revise the definition of MSMEs in the Act on two earlier occasions. The government introduced the MSME Development (Amendment) Bill, 2015 which proposed to increase the investment limits for manufacturing and services MSMEs.[3] This Bill was withdrawn in July 2018 and another Bill was introduced. The MSME Development (Amendment) Bill, 2018 proposed to: (i) use annual turnover as criteria instead of investment for classification of MSMEs, (ii) remove the distinction between manufacturing and services, and (iii) provide the central government with the power to revise the turnover limits, through a notification.[4] The 2018 Bill lapsed with the dissolution of 16th Lok Sabha.

Global trends in criteria for the classification of MSMEs
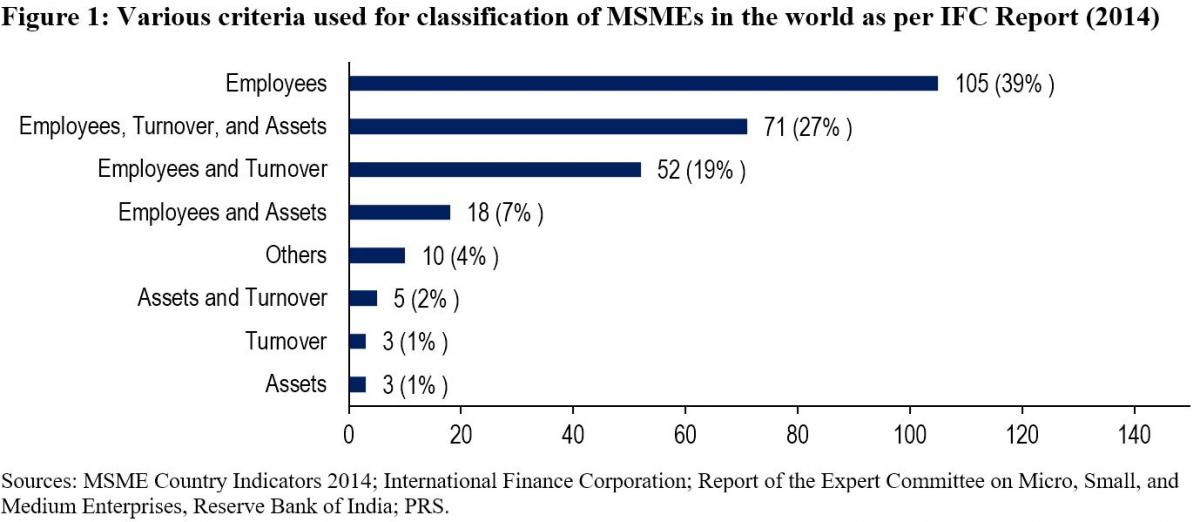
While India will now be using investment and annual turnover as the criteria to classify MSMEs, globally, the number of employees is the most widely used criteria for classifying MSMEs. The Reserve Bank of India's Expert Committee on MSMEs (2019) cited a study by the International Finance Corporation in 2014 which analysed 267 definitions used by different institutions in 155 countries.[5],[6] According to the study, countries used a combination of criteria to classify MSMEs. 92% of the definitions used the number of employees as one of the criteria. Other frequently used criteria were: (i) turnover (49%), and (ii) value of assets (36%). 11% of the analysed definitions used alternative criteria such as: (i) loan size, (ii) years of experience, and (iii) initial investment.

Evaluation of common criteria used to define MSMEs
Investment: The 2006 Act uses investment in plant, machinery, and equipment to classify MSMEs. Some of the issues with the investment criteria include:
Due to their informal and small scale of operations, firms often do not maintain proper books of accounts and hence find it difficult to get classified as MSMEs as per the current definition.5
The investment-based classification incentivises promoters to keep the investment size restricted to retain the benefits associated with the micro or small category.7
Turnover: The 2018 Bill sought to replace the investment criteria with annual turnover as the sole criteria for the classification of MSMEs. The Standing Committee agreed with the proposal under the Bill to use annual turnover as the criteria instead of investment.7 It observed that this could overcome some of the shortcomings of classification based on investment. While turnover based criteria will also require verification, the Committee noted that the GST Network (GSTN) data can act as a reliable source of information for this purpose. However, it also observed that:7
With turnover as a criterion for classification, corporates may misuse the incentives meant for MSMEs. For instance, there is a possibility that a multi-national company may produce a large quantity of products worth a high turnover and then market it through various subsidiaries registered as Micro or Small enterprise under GSTN.
The turnover of some enterprises may fluctuate depending on their business, which may result in the change of classification of the enterprise during a year.
The Committee noted that there is a wide gap in turnover limits. For instance, an enterprise with a turnover of Rs 6 crore and an enterprise with a turnover of Rs 75 crore (as proposed in 2018 Bill) would both be classified as a small enterprise, which seems incongruous.
The Expert Committee (RBI) also recommended using annual turnover as the criteria for classification instead of investment.5 It observed that turnover based definition would be transparent, progressive, and easier to implement through the GSTN. It also recommended that the power to change the definition of MSMEs should be delegated to the executive as it will help in responding to changing economic scenarios.
Number of employees: The Standing Committee had highlighted that in a labour-intensive country like India, appropriate focus is required on employment generation and MSME sector is the most suitable platform for this.7 It had recommended that the central government should assess the number of persons employed in the MSME sector and also consider employment as a criterion while classifying MSMEs. However, the Expert Committee (RBI) stated that while the employment-based definition is an additional feature preferred in some countries, the definition would pose challenges in implementation.5 According to the Ministry of MSME, employment as a criterion has problems due to: (i) factors such as seasonality and informal nature of engagement, (ii) similar to investment criteria, this would also require physical verification and has associated cost overheads.7
Number of MSMEs
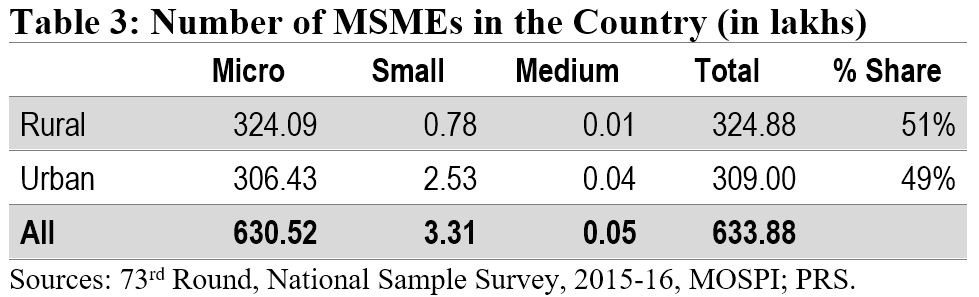
According to the National Sample Survey (2015-16), there were around 6.34 crore MSMEs in the country. The micro sector with 6.3 crore enterprises accounted for more than 99% of the total estimated number of MSMEs. The small and medium sectors accounted for only 0.52% and 0.01% of the estimated number of enterprises, respectively. Another dataset to understand the distribution of MSMEs is Udyog Aadhaar, a unique identity provided by the Unique Identification Authority of India (UIDAI) to MSME enterprises.[8] Udyog Aadhaar registration is based on self-declaration by enterprises. Between September 2015 and June 2020, 98.6 lakh enterprises have registered with UIDAI. According to this dataset, micro, small, and medium enterprises comprise 87.7%, 11.8% and 0.5% of the MSME sector respectively.
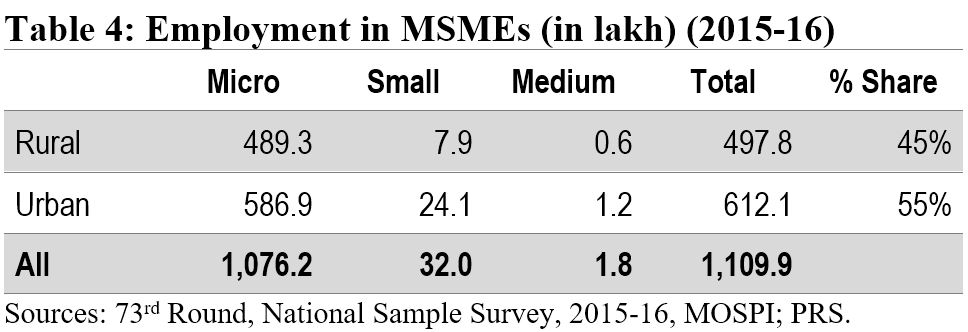
Employment in the MSME sector
The MSME sector employed nearly 11.1 crore people in 2015-16. The sector was the second largest employer after the agriculture sector. The highest number of employed persons were engaged in trade activity (35%), followed by persons engaged in manufacturing (32%).
Implications of change in the definition of MSMEs
The change in the definition of MSMEs may result in many enterprises which are currently classified as Small enterprises be reclassified as Micro, and those classified as Medium enterprises be reclassified as Small. Further, there may be many enterprises which are not currently classified as MSMEs, which may fall under the MSME classification as per the new definition. Such enterprises will also now benefit from the schemes related to MSMEs. The Ministry of MSME runs various schemes to provide for: (i) flow of credit to MSMEs, (ii) support for technology upgrade and modernisation, (iii) entrepreneurship and skill development, and (iv) cluster-wise measures to promote capacity-building and empowerment of MSME units. For instance, under the Credit Guarantee Fund Scheme for Micro and Small Enterprises, a credit guarantee cover of up to 75% of the credit is provided to micro and small enterprises.[9] Thus, the re-classification may require a significant increase in budgetary allocation for the MSME sector.
Other announcements related to MSMEs in the aftermath of COVID-19
MSME sector accounted for nearly 33.4% of the total manufacturing output in 2017-18.[10] During the same year, its share in the country’s total exports was around 49%. Between 2015 and 2017, the contribution of the sector in GDP has been around 30%. Due to the national lockdown induced by COVID-19, businesses including MSMEs have been badly hit. To provide immediate relief to the MSME sector, the government announced several measures in May 2020.[11] These include: (i) collateral-free loans for MSMEs with up to Rs 25 crore outstanding and up to Rs 100 crore turnover, (ii) Rs 20,000 crore as subordinate debt for stressed MSMEs, and (iii) Rs 50,000 crore of capital infusion into MSMEs. These measures have also been approved by the Union Cabinet.[12]
For more details on the announcements made under the Aatma Nirbhar Bharat Abhiyan, see here.
[1] “Cabinet approves Upward revision of MSME definition and modalities/ road map for implementing remaining two Packages for MSMEs (a)Rs 20000 crore package for Distressed MSMEs and (b) Rs 50,000 crore equity infusion through Fund of Funds”, Press Information Bureau, Cabinet Committee on Economic Affairs, June 1, 2020.
[2] The Micro, Small and Medium Enterprises Development Act, 2006, https://samadhaan.msme.gov.in/WriteReadData/DocumentFile/MSMED2006act.pdf.
[3] The Micro, Small and Medium Enterprises Development (Amendment) Bill, 2015, https://www.prsindia.org/sites/default/files/bill_files/MSME_bill%2C_2015_0.pdf.
[4] The Micro, Small and Medium Enterprises Development (Amendment) Bill, 2018, https://www.prsindia.org/sites/default/files/bill_files/The%20Micro%2C%20Small%20and%20Medium%20Enterprises%20Development%20%28Amendment%29%20Bill%2C%202018%20Bill%20Text.pdf.
[5] Report of the Expert Committee on Micro, Small and Medium Enterprises, The Reserve Bank of India, July 2019, https://rbidocs.rbi.org.in/rdocs/PublicationReport/Pdfs/MSMES24062019465CF8CB30594AC29A7A010E8A2A034C.PDF.
[6] MSME Country Indicators 2014, International Finance Corporation, December 2014, https://www.smefinanceforum.org/sites/default/files/analysis%20note.pdf.
[7] 294th Report on Micro Small and Medium Enterprises Development (Amendment) Bill 2018, Standing Committee on Industry, Rajya Sabha, December 2018, https://rajyasabha.nic.in/rsnew/Committee_site/Committee_File/ReportFile/17/111/294_2019_3_15.pdf.
[8] Enterprises with Udyog Aadhaar Number, National Portal for Registration of Micro, Small & Medium Enterprises, Ministry of Micro, Small and Medium Enterprises, https://udyogaadhaar.gov.in/UA/Reports/StateBasedReport_R3.aspx.
[9] Credit Guarantee Fund Scheme for Micro and Small Enterprises, Ministry of Micro, Small and Medium Enterprises, http://www.dcmsme.gov.in/schemes/sccrguarn.htm.
[10] Annual Report 2018-19, Ministry of Micro, Small and Medium Enterprises, https://msme.gov.in/sites/default/files/Annualrprt.pdf.
[11] "Finance Minister announce measures for relief and credit support related to businesses, especially MSMEs to support Indian Economy’s fight against COVID-19", Press Information Bureau, Ministry of Finance, May 13, 2020.
[12] "Cabinet approves additional funding of up to Rupees three lakh crore through introduction of Emergency Credit Line Guarantee Scheme (ECLGS)", Press Information Bureau, Ministry of Finance, May 20, 2020.
Recently, the Standing Committee on Health and Family Welfare submitted its report to the Parliament on the National Commission for Human Resource for Health Bill, 2011. The objective of the Bill is to “ensure adequate availability of human resources in the health sector in all states”. It seeks to set up the National Commission for Human Resources for Health (NCHRH), National Board for Health Education (NBHE), and the National Evaluation and Assessment Council (NEAC) in order to determine and regulate standards of health education in the country. It separates regulation of the education sector from that of professions such as law, medicine and nursing, and establishes professional councils at the national and state levels to regulate the professions. See here for PRS Bill Summary. The Standing Committee recommended that this Bill be withdrawn and a revised Bill be introduced in Parliament after consulting stakeholders. It felt that concerns of the professional councils such as the Medical Council of India and the Dental Council of India were not adequately addressed. Also, it noted that the powers and functions of the NCHRH and the National Commission on Higher Education and Research (to be established under the Higher Education and Research Bill, 2011 to regulate the higher education sector in the country) were overlapping in many areas. Finally, it also expressed concern over the acute shortage of qualified health workers in the country as well as variations among states and rural and urban areas. As per the 2001 Census, the estimated density of all health workers (qualified and unqualified) is about 20% less than the World Health Organisation’s norm of 2.5 health workers per 1000 population. See here for PRS Standing Committee Summary. Shortfall of health workers in rural areas Public health care in rural areas is provided through a multi-tier network. At the lowest level, there are sub health-centres for every population of 5,000 in the plains and 3,000 in hilly areas. The next level consists of Primary Health Centres (PHCs) for every population of 30,000 in the plains and 20,000 in the hills. Generally, each PHC caters to a cluster of Gram Panchayats. PHCs are required to have one medical officer and 14 other staff, including one Auxiliary Nurse Midwife (ANM). There are Community Health Centres (CHCs) for every population of 1,20,000 in the plains and 80,000 in hilly areas. These sub health centres, PHCs and CHCs are linked to district hospitals. As on March 2011, there are 14,8124 sub health centres, 23,887 PHCs and 4809 CHCs in the country.[i] Sub-Health Centres and Primary Health Centres
Table 1: State-wise comparison of vacancy in PHCs
|
Doctors at PHCs |
ANM at PHCs and Sub-Centres |
|||||
| State | Sanctioned post | Vacancy | % of vacancy | Sanctioned post | Vacancy | % of vacancy |
| Chhattisgarh | 1482 | 1058 | 71 | 6394 | 964 | 15 |
| West Bengal | 1807 | 801 | 44 | 10,356 | NA | 0 |
| Maharashtra | 3618 | 1326 | 37 | 21,122 | 0 | 0 |
| Uttar Pradesh | 4509 | 1648 | 36 | 25,190 | 2726 | 11 |
| Mizoram | 57 | 20 | 35 | 388 | 0 | 0 |
| Madhya Pradesh | 1238 | 424 | 34 | 11,904 | 0 | 0 |
| Gujarat | 1123 | 345 | 31 | 7248 | 817 | 11 |
| Andaman & Nicobar Isld | 40 | 12 | 30 | 214 | 0 | 0 |
| Odisha | 725 | 200 | 28 | 7442 | 0 | 0 |
| Tamil Nadu | 2326 | 622 | 27 | 9910 | 136 | 1 |
| Himachal Pradesh | 582 | 131 | 22 | 2213 | 528 | 24 |
| Uttarakhand | 299 | 65 | 22 | 2077 | 0 | 0 |
| Manipur | 240 | 48 | 20 | 984 | 323 | 33 |
| Haryana | 651 | 121 | 19 | 5420 | 386 | 7 |
| Sikkim | 48 | 9 | 19 | 219 | 0 | 0 |
| Meghalaya | 127 | 23 | 18 | 667 | 0 | 0 |
| Delhi | 22 | 3 | 14 | 43 | 0 | 0 |
| Goa | 46 | 5 | 11 | 260 | 20 | 8 |
| Karnataka | 2310 | 221 | 10 | 11,180 | 0 | 0 |
| Kerala | 1204 | 82 | 7 | 4232 | 59 | 1 |
| Andhra Pradesh | 2424 | 76 | 3 | 24,523 | 2876 | 12 |
| Rajasthan | 1478 | 6 | 0.4 | 14,348 | 0 | 0 |
| Arunachal Pradesh | NA | NA | NA | NA | NA | 0 |
| Assam | NA | NA | NA | NA | NA | 0 |
| Bihar | 2078 | 0 | NA | NA | NA | 0 |
| Chandigarh | 0 | 0 | NA | 17 | 0 | 0 |
| Dadra & Nagar Haveli | 6 | 0 | NA | 40 | 0 | 0 |
| Daman & Diu | 3 | 0 | NA | 26 | 0 | 0 |
| Jammu & Kashmir | 750 | 0 | NA | 2282 | 0 | 0 |
| Jharkhand | 330 | 0 | NA | 4288 | 0 | 0 |
| Lakshadweep | 4 | 0 | NA | NA | NA | 0 |
| Nagaland | NA | NA | NA | NA | NA | 0 |
| Puducherry | 37 | 0 | NA | 72 | 0 | 0 |
| Punjab | 487 | 0 | NA | 4044 | 0 | 0 |
| Tripura | NA | NA | NA | NA | NA | 0 |
| India | 30,051 | 7,246 | 24 | 1,77,103 | 8,835 | 5 |
| Sources: National Rural Health Mission (available here), PRS.Note: The data for all states is as of March 2011 except for some states where data is as of 2010. For doctors, these states are Bihar, UP, Mizoram and Delhi. For ANMs, these states are Odisha and Uttar Pradesh. | ||||||
Community Health Centres
Table 2: Vacancies in CHCs of medical specialists
| Surgeons | Gynaecologists | Physicians | Paediatricians | |
| State |
% of vacancy |
|||
| Andaman & NicobarIsland | 100 | 100 | 100 | 100 |
| Andhra Pradesh | 74 | 0 | 45 | 3 |
| Arunachal Pradesh | NA | NA | NA | NA |
| Assam | NA | NA | NA | NA |
| Bihar | 41 | 44 | 60 | 38 |
| Chandigarh | 50 | 40 | 50 | 100 |
| Chhattisgarh | 85 | 85 | 90 | 84 |
| Dadra & Nagar Haveli | 0 | 0 | 0 | 0 |
| Daman & Diu | 0 | 100 | 0 | 100 |
| Delhi | 0 | 0 | 0 | 0 |
| Goa | 20 | 20 | 67 | 66 |
| Gujarat | 77 | 73 | 0 | 91 |
| Haryana | 71 | 80 | 94 | 85 |
| Himachal Pradesh | NA | NA | NA | NA |
| Jammu & Kashmir | 34 | 34 | 53 | 63 |
| Jharkhand | 45 | 0 | 81 | 61 |
| Karnataka | 33 | NA | NA | NA |
| Kerala | NA | NA | NA | NA |
| Lakshadweep | 0 | 0 | 100 | 0 |
| Madhya Pradesh | 78 | 69 | 76 | 58 |
| Maharashtra | 21 | 0 | 34 | 0 |
| Manipur | 100 | 94 | 94 | 87 |
| Meghalaya | 50 | NA | 100 | 50 |
| Mizoram | NA | NA | NA | NA |
| Nagaland | NA | NA | NA | NA |
| Odisha | 44 | 45 | 62 | 41 |
| Puducherry | 0 | 0 | 100 | NA |
| Punjab | 16 | 36 | 40 | 48 |
| Rajasthan | 57% | 46 | 49 | 24 |
| Sikkim | NA | NA | NA | NA |
| Tamil Nadu | 0 | 0 | 0 | 0 |
| Tripura | NA | NA | NA | NA |
| Uttar Pradesh | NA | NA | NA | NA |
| Uttarakhand | 69 | 63 | 74 | 40 |
| West Bengal | 0 | 57 | 0 | 78 |
| India | 56 | 47 | 59 | 49 |
| Sources: National Rural Health Mission (available here), PRS. | ||||
[i]. “Rural Healthcare System in India”, National Rural Health Mission (available here).

